Your ₹500 multivitamin has a problem nobody on the packaging mentions.
By Soham Shinde
6/19/20263 min read


A few months ago I did something I should have done much earlier: I read the full ingredient list on a multivitamin I'd been taking for a year.
Not the "what it contains" front panel. The actual form of each ingredient. Magnesium oxide. Cyanocobalamin. Ferrous sulphate. Cholecalciferol.
I then looked up the bioavailability of each of those forms.
Magnesium oxide: approximately 4% bioavailability. I was taking 100mg per day and absorbing roughly 4mg. The daily requirement is around 400mg.
I'd spent the better part of a year taking a supplement that was, in practical terms, doing almost nothing for my magnesium levels. The bottle said "Contains Magnesium." It did. Just not in a form my gut could meaningfully absorb.
This is the bioavailability problem. And it's almost never talked about.
What bioavailability actually means
Bioavailability is the percentage of a nutrient that actually enters your bloodstream and reaches the tissues that need it. It's not the same as what's listed on the label.
A tablet can contain 500mg of vitamin C. But if your gut absorbs 80% of it, your effective dose is 400mg. If it only absorbs 20%, your effective dose is 100mg. The number on the label tells you what went in the mouth. Bioavailability tells you what actually got used.
Most multivitamin labels tell you nothing about bioavailability. They're not required to. And most consumers assume that milligrams in equals milligrams absorbed. It doesn't.
The form problem — same nutrient, radically different absorption
For most vitamins and minerals, the chemical form matters enormously. Here are the most important ones to know:
Magnesium
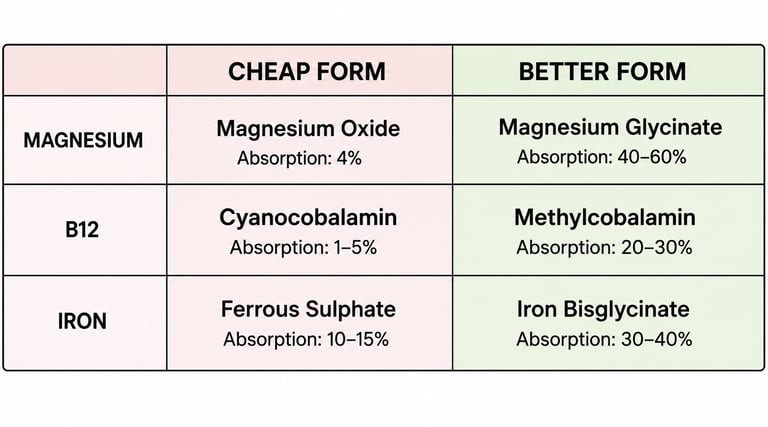
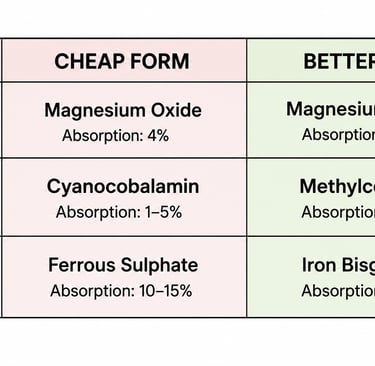
• Magnesium oxide: ~4% bioavailability. Cheapest form. Used in most budget multivitamins.
• Magnesium citrate: ~25-30% bioavailability. Much better absorbed.
• Magnesium glycinate: ~50-80% bioavailability. Best absorbed form for most people. Also gentler on the gut.
Vitamin B12
• Cyanocobalamin: Synthetic form. Requires conversion in the body before use. Poorly absorbed at low doses.
• Methylcobalamin: Active form. Used directly by the body. Significantly better absorbed, especially sublingually.
This distinction is particularly important for vegetarians and vegans, who depend entirely on supplementation for B12 and often find standard supplements insufficient.
Iron
• Ferrous sulphate: High iron content but causes significant GI distress in many people and is poorly absorbed on a full stomach.
• Ferrous bisglycinate: Better tolerated, better absorbed, and can be taken with food.
The nutrient competition problem
Even if a multivitamin uses good forms of each nutrient, there's a second problem: minerals compete with each other for the same absorption transporters in your gut.
Calcium and magnesium compete. Iron and zinc compete. High-dose calcium can suppress zinc and magnesium absorption when taken simultaneously. A multivitamin that packs calcium, magnesium, zinc, and iron into the same tablet is creating conditions where these nutrients actively work against each other.
This is why some nutritionists recommend taking calcium and magnesium at different times of day, and why iron is often better absorbed when taken separately from other minerals.
What the large-scale research actually says
A 2022 Cochrane review — the gold standard of evidence synthesis — found no convincing evidence that multivitamin supplementation reduces mortality, cardiovascular disease, or cancer risk in adults without diagnosed deficiencies. A 2023 analysis in the Annals of Internal Medicine reached the same conclusion.
This isn't an anti-supplement position. It's a precision argument: multivitamins as a concept — 22 nutrients in one tablet, taken prophylactically by people who haven't tested for deficiencies — have poor evidence behind them. Targeted supplementation for a confirmed deficiency, using the right form and dose, has strong evidence.
The difference between those two things is a blood test and 10 minutes of reading.
What I actually do now
I got a blood panel. Found I was deficient in D3 and had suboptimal B12. I now take D3 + K2 (cholecalciferol form) and methylcobalamin B12 — sublingual, not tablet. Both targeted. Both the right form. Both based on a blood result, not a guess.
I stopped the multivitamin.
Key Takeaways
• Bioavailability = how much of a nutrient your body actually absorbs — very different from label numbers
• Magnesium oxide has ~4% absorption. Magnesium glycinate has ~50-80%
• B12 as methylcobalamin absorbs significantly better than cyanocobalamin
• Minerals in the same tablet compete for absorption — calcium blocks magnesium and zinc
• Large RCTs show no mortality benefit from multivitamins in people without diagnosed deficiencies
• Get a blood test. Supplement specifically. Use the right form.
SOURCES
Cochrane Review (2022) — Vitamins and minerals for the primary prevention of cardiovascular disease and cancer
Annals of Internal Medicine (2023) — Dietary supplements in adults: a systematic review
NIH Office of Dietary Supplements — Magnesium fact sheet
Journal of Nutritional Biochemistry — Mineral absorption competition in the human intestine